A patient story we would like to share with you features one of our Patient Ambassadors, Megan Burns, from Greater Chicago.
Before her injury, Megan was a healthy active adult in her early thirties. Megan enjoyed playing tennis a few times a week at her neighborhood courts in the summer. On Sundays, Megan would play golf with her partner Brian and her Aunt and Uncle. She also went on daily walks with her dog Chip. Megan and Brian also enjoyed hiking in Lake Geneva on the scenic lake path in the spring, summer, and fall in Wisconsin.
Megan also liked a little adventure. Shortly before her injury she hiked up the Devils Doorway at Devil’s Lake in Wisconsin, enjoyed zip lining down mountains in the Jamaican rainforest, and walked up the 600-foot-long landmark Dunn’s River waterfall. Every May, Megan and her cousin Mindy would go for an adrenaline rush and ride all the big roller coasters at Six Flags Great America; rain or shine!
Megan’s entire life changed in December of 2015 when she had a stroke in her spinal cord caused by a ruptured arteriovenous malformation (AVM). A spinal AVM is a rare, abnormal tangle of blood vessels on, in, or near the spinal cord. Due to the spinal cord stroke, Megan underwent a resectioning of her spinal cord which was performed in February of 2016. After her AVM and resectioning surgery, Megan was diagnosed with a T-12- incomplete spinal cord injury (iSCI).
Post-injury, Megan used a wheelchair to get around. Over time with physical therapy and lots of hard work, she was able to progress to walking with a wheeled walker and eventually a straight cane and AFO (ankle foot orthoses) braces. Doctors were thrilled with this progress since her original prognosis was that she would always need to use a wheelchair. Although the progress was great, Megan did not accept that she had reached the end of her journey towards walking independently. She would rely on her cane for stability and drag her legs through the motions of walking. For Megan, this was not the best solution and was not the peak of her progress!
Megan was introduced to Ekso in the fall of 2017 which was two years after her injury. Still not satisfied with the quality of her gait, she went to the Shirley Ryan AbilityLab website to look for rehabilitation help. Megan saw they were seeking participants for a study called WISE (Walking Improvement for SCI with Exoskeleton) which was looking at comparing Ekso rehab with traditional rehab for incomplete spinal cord injured patients. She fit the study criteria and signed up immediately. Luckily, Megan started as a participant of the trial in the first quarter of 2018. She would end up using Ekso three days per week for twelve weeks and here is what happened next:
First session – Megan found her balance with the help of the preGait functions and her posture began to recover.
Third session – She became very comfortable and confident in the device. Megan learned how to work together with the exoskeleton, that Ekso was not walking for her, and stopped fighting it. At this point she really started to learn from it.
“It was here that I realized I need to take the information I learned in Ekso and carry it over into real life. This is where I realized the importance of Ekso and the steps. I was taking 500+ steps in my first few sessions of 45 minutes each. That was more steps than I was taking in days. Not only was I thrilled at the step quantity, but also the quality. The step pattern in Ekso is natural and would not allow me to drag my toes. You can only take quality steps in the device.”
Fifth session – Together with her therapist, Megan realized she had not used her calves in two years. She finally started pushing with her calves again to clear the toes that were curled under from foot drop. Even today, Megan says, “I still hear my PT when I am walking to PUSH.”
Session twelve – Megan stopped using her AFO because she was engaging her calves with every step. By the twelfth session she was taking 900+ steps in Ekso each time, including backward and forward walking.
By session twenty Megan was walking in the community completely unassisted—no more cane!
And the best news of all, by the thirty-sixth session in Ekso Megan was back to golfing, a goal of hers since her injury back in late 2015.
“Now, in outpatient, my therapists are kind and patient, but also challenge me. MidAmerica Rehabilitation Hospital is now my family.”
Today, Megan still can’t feel her legs from the waist down but has been able to build up her muscles in her legs in order to keep walking. She has carried on with all the lessons from her Ekso training and has been walking unassisted for nearly two years! She has returned to using Ekso in the outpatient setting, for what she calls “tune ups”. As a busy professional and someone who travels for pleasure as often as she can, Megan tends to get busy with life moving quickly and returns to some old habits—short steps, not weight-shifting, and dragging her toes.
“Every time I use Ekso I learn something new and take it with me. I do have to think of every step I am going to take, but now it is so much easier.”
Megan would like to stress how much she believes in Ekso. So much so, that she would drive more than two hours round-trip for the twelve-week duration of the study to get into the device to keep learning to walk. We are so thrilled with Megan’s progress and her incredible return to the full life she was enjoying prior to her injury. Since regaining her balance and strength she has been able to get back to her adventurous side and has been parasailing, scuba diving, cliff jumping, and hiking at the Grand Canyon. She also has returned to joining friends for concerts and still makes her annual trip to Six Flags to ride the roller coasters with her cousin.
Megan’s success with Ekso has also led to her joining Ekso Bionics as a Patient Ambassador so she can continue to share her story with as many people as possible and spread hope.
Whether you are lifting heavy objects or completing light and repetitive tasks, construction exoskeletons are your best chance of injury prevention and productivity enhancement. In 2017 alone, there were at least 12,000 injuries per month in the construction industry (1), many of which could have been prevented with the use of exoskeletons. According to research (2), exoskeletons reduce human metabolic cost and thermophysiological response during upper-body work tasks, which translates to less fatigue and strain for workers., resulting in increased productivity. For construction and warehouse workers, exoskeletons are the next industrial shift that will lead to increased efficiency and productivity.
In this article, you will learn what exoskeletons are, how they are applied in construction, and their benefits. Let’s dive in.
What Are Exoskeletons?
Exoskeletons, also referred to as exosuits, powered-armor, or exo frames, are wearable external frames that offer extra support and enhance a person’s biomechanical capabilities. Think Iron Man from the Avengers, but in real life. The exoskeleton acts as a strength amplifier that augments physical performance or a corrective device for restoring mobility.
Some people believe that exoskeletons are a new “thing”. However, this technology has been in existence since 1890 but has only gained more traction in recent years due to accelerated technology developments. The early model, designed and patented by Nicholas Yagn (3), was a spring-operated device that enhanced the user’s ability to run and jump.
Today, exoskeletons have wide applications and are used in the military, medical, and construction fields. In the medical industry, physical therapists use them as locomotive assistance and gait training devices for patients who have a condition or injury that affects mobility. While in the construction industry, they are primarily used to help workers with their upper extremity mobility by reducing strain and increasing productivity.
There are two types of exoskeletons, powered and passive. A powered exoskeleton contains electric motors, levers, hydraulics, and other technologies that enable limb mobility with increased endurance and strength. It works by sensing the wearer’s motions, sending signals to the motors, and offering the necessary support. A passive exoskeleton differs from a powered exoskeleton because it is purely mechanical. However, they both offer benefits such as shoulder, waist, or thigh support. Additionally, it offers movement assistance when lifting heavy items. Powered exoskeletons are mostly used in military and physical therapy, while passive exoskeletons are more commonly used in construction and other industrial industries.
Exoskeletons and Injury in the Construction Industry
Did you know that the rate of work-related musculoskeletal disorders in construction is 16% higher than in all industries combined?(4) This statistic alone should be enough to point you to the most significant challenge that construction workers face: workplace injury. According to the Construction Chartbook (5), the most common injuries in construction are located in the back, shoulders, and other joints. This can be attributed to the long and repetitive tasks that eventually lead to overexertion and strain to workers’ bodies.
“The most common cause of workplace injuries was overexertion and fatigue. With 20% of construction workers reporting severe pain, construction workers are five times more likely to report poor health. US companies pay nearly $62 billion per year for workplace injuries.”(6)
Workplace injury results in lower productivity, which accumulates to more than 104 million lost production days.(1) In addition, it impacts construction workers’ morale as the uninjured employees have to take up bigger workloads to make up for the injured and recuperating workers. It also affects the injured person’s ability to complete future tasks and lowers their working lifespan.. However, organizations can avoid this by investing in construction exoskeletons.
In a study conducted in 2015 on the application of exoskeletons in industrial applications and their potential effects on physical workload, researchers discovered that exoskeletons greatly reduce fatigue while improving endurance (7). Additionally, exoskeletons reduce shoulder discomfort, thereby improving work quality and productivity among workers. Apart from decreasing the risk of workplace injury, exoskeletons also assist aging workers, and give them an opportunity to work beyond their age and physical limit.
Construction exoskeletons are the future of the construction industry due to the efficiency and productivity opportunities they present. Their primary purpose being: to improve the quality of life for construction workers and prevent injury.
You can use exoskeletons on the manufacturing floor to engage in long-intensive overhead work like installing sensors and filters without straining or injuring yourself. Benefits include joint support that’ll boost your endurance, productivity and prevent injury.
The Construction Exoskeleton Vest
Construction exoskeletons come in different shapes and variations suited to a specific task. Depending on the workload, it can be a full suit, a simple vest to support upper limb mobility or just a glove. Let’s take a look into an exoskeleton vest.
The construction exoskeleton vest is an upper-body exosuit specifically designed to support upper extremity mobility. Its main goal is to reduce workplace injury and worker fatigue by supporting muscle activity and joint movement. It also reduces discomfort when performing repetitive overhead tasks. Let’s establish one important fact; a construction exoskeleton won’t give you ‘Iron Man-level’ superhuman strength. In essence, the vest serves to reduce musculoskeletal loads. You’ll still lift an equal amount of load as you could before. The only difference will be that the load will be lighter and easier to carry since you’ll have additional muscle support.
The construction exoskeleton vest contains features like:
Lightweight frame: This makes it easy and comfortable to wear.
Durable materials: The vest is built for the construction environment where they can be exposed to the harshest element and function fully without breakage.
Assistive: The Exo suit has an adjustable force assistance level that allows you to determine the amount of arm support you want from the suit.
Natural-tracking: You can wear the suit and move naturally using your intuition, instincts, and reflexes to control it.
Minimal contact points: This allows workers to work unhindered with a full range of motion and great airflow for comfort.
How Does The Construction Exoskeleton Vest Work?
Exosuits work in different ways depending on how they are powered. Mechanical exoskeletons, which do not use electricity, take weight from certain parts of the body and redistribute it to other areas. For instance, it can take weight from the arms or back when doing tedious overhead work and transfer it to your core to reduce fatigue and strain on muscles and joints. Mechanical exoskeletons are more advantageous since they don’t need to be recharged to use them. So, there’s no downtime. Additionally, they offer more longevity.
On the other hand, electric exoskeletons are more powerful and can handle more weight. They work by increasing pressure and strength in targeted areas as required. The frame responds to the wearer’s motion and provides support when needed. Due to their reliance on power, they can stop work if they run out of charge. In addition, you have to recharge them between uses.
The construction exoskeleton vest is one of the must-have technologies for construction, logistics, and warehouse workers, and for manufacturers who are interested in increasing occupational safety. It is the best solution to reducing muscle pulls, elbow and spinal injuries, and back sprains. It represents the coming together of man and machine to make work easier and more efficient. Let’s dive into the benefits more extensively below.
Fun Fact: The Master Mystery, released in 1919, is the first movie to feature a powered exoskeleton
5 Benefits Of Construction Exoskeletons
You can enjoy many benefits from using industrial exoskeletons, like lifting heavy loads, performing repetitive tasks, reducing the risk of injuries, supporting joints, and increasing work efficiency.
Injury and Strain Prevention
Exoskeletons cut down on overexertion by supporting workers’ upper limbs when performing monotonous activities. They distribute the user’s weight evenly to the core and waist by reducing strain on the arms and shoulders. This leads to decreased workplace injuries like back sprains and shoulder injuries.
Withstanding Repetitive Tasks
Picture a construction worker who has to raise their arms over their heads for hours on end plastering a wall or installing drywall. That’s a daunting task, but with a construction exoskeleton, their workload is made more bearable because they have extra support for their arms. They no longer have to go home with joint and back pains, and they can work for more hours without overexerting themselves and thereby increasing their productivity.
Increased Productivity
Exoskeletons have been proven to increase workers’ endurance by reducing the amount of energy exerted on repetitive tasks. Additionally, since the frame takes on a portion of the musculoskeletal load, it reduces strain on the worker’s muscles and lowers fatigue. Coupled with less injury and strain, this becomes a great productivity enhancer for workers since they can work longer and more efficiently.
More Work Accuracy
After endless hours of overhead work, accuracy is lowered due to muscle fatigue and exhaustion. However, with an exosuit, you can practically maintain most of your attention and focus on the task at hand without the distraction of strain and fatigue.
More Opportunities For Aged Contractors
Due to the labor-intensive nature of construction work, older contractors are more likely to be limited by their physical abilities. But with a construction exoskeleton, these workers are able to handle more strenuous work effectively.
Conclusion
In recent years, the construction industry has experienced a lot of automation. However, not every task can be automated and replaced with a robot. There are specific, heavy and repetitive tasks that only humans can do. And the best option for attaining more efficiency and productivity in these non-autonomous tasks is to invest in well-produced exoskeletons. They are an innovative injury prevention solution and present great productivity potential in the construction industry.
If you are considering getting a construction exoskeleton, Ekso Bionics is your best choice. We are the leading company in exoskeleton technologies and have produced some of the best products in the world for the last 17 years. We’ve worked with the United States military, DARPA, Johns Hopkins, Shirley Ryan AbilityLab, Kessler Institute, the Department for Veterans Affairs, and UCLA, among others. Our products are FDA-Approved and are based on clinical experts and feedback from industry leaders.
Every year, 55.9 million people suffer from an acquired brain injury (ABI), which is any injury to the brain that is not hereditary, congenital, degenerative, or induced by birth trauma. 15 million suffer from strokes, or cerebral vascular accident (CVA)—the fifth leading cause of death in the United States and a major cause of long-term disability. A stroke results when part of their brain is deprived of oxygen caused by a blood clot blocking blood flow or by a rupture in the artery feeding blood to a part of the brain. Up to 500,000 people suffer from spinal cord injury (SCI), classified by decrease or complete loss of sensation and/or movement below the level of injury.
As a result, those with an ABI, CVA, or SCI may be left with limited mobility or some form of paralysis. This can be a devastating diagnosis that is completely life-changing for patients and their families.
Human robotic exoskeletons offer a new, promising approach to restoring mobility after such injuries. Health experiences including regained mobility, as well as improved oxygen intake, bowel and bladder function, joint maintenance, circulation, and easement of pain have been shown in patients using robotic exoskeletons. With the use of human robotic exoskeletons, patients who are working with physical therapists can regain basic movements or even develop the ability to walk again independently.
What are Exoskeletons?
Robotic exoskeletons are wearable devices made of mechanical and sometimes electrical technologies that are used to enhance the physical performance of the wearer or act as orthotic devices for gait rehabilitation or locomotion assistance. Depending on the purpose they serve, human robotic exoskeletons can be made from materials such as carbon fiber and metal, or they can be made entirely out of soft and elastic parts. Some exoskeletons need to be tailored to the individual that is using them and have adjustable hardware to fulfill that need. Overall, the technology behind the exoskeleton depends largely on its type and function.
Exoskeletons can be considered powered, using technology like sensors and actuators, or passive, using purely mechanical parts. The electronics with which powered exoskeletons are equipped register how much force is being applied to any given action, allowing the exoskeleton to share some of that burden with the user. Passive exoskeletons take the weight from the body’s extremities and distribute it to the core or leg muscles, spreading the weight out to relieve pressure from the targeted body part. This prevents fatigue from occurring as quickly and lowers the chances of strain or injury.
Groups That Benefit From Exoskeletons
Human robotic exoskeletons can be used for the purpose of health, industrial labor, and military research and development. For health, exoskeletons can be used to restore someone’s limb functionality and help them to walk again.
Instances of health-related applications for exoskeletons include stroke, spinal cord injury, acquired and traumatic brain injury, muscular dystrophy, cerebral palsy, orthopedic injury, Guillain barre, brachial plexus injuries, multiple sclerosis. These diagnoses can result in a range of impairments including monoplegia, hemiplegia, paraplegia, quadriplegia, ataxia, and other weaknesses. Benefits of exoskeletons used in the healthcare field include: increased user independence, decreased chronic pain, reduction of energy required for movement, increased range of motion and endurance, increased quality of life, and more.
Patients with lower extremity mobility loss can enlist the help of lower body exoskeletons to address gait inefficiencies by supporting the spine, trunk, and legs including hip, knee, and ankle joints. In this instance, the exoskeleton promotes correct movement patterns in all phases of physical rehabilitation and challenges patients as they progress towards walking back into their communities.
Patients with upper extremity mobility loss can wear upper-extremity exoskeletons designed to assist their affected shoulder and arm during rehabilitation, resulting in rehabilitation sessions with a higher dosage, more intense therapy, and a wider active range of motion. An exoskeleton can provide access to the shoulder joint and scapula to help therapists facilitate movement while the device supports the patient’s arm with minimal interference, allowing for a natural motion.
For patients with acquired brain injury and stroke, lower-extremity robotic exoskeletons are utilized by physical therapists to improve patients’ orientation to midline, weight shift, stepping quality, and lower extremity muscle strength. These exoskeletons utilize the principles of neuroplasticity to help physical therapists deliver high quality, intense, repetitive, task-specific practice to patients on their journey of reclaiming independence.
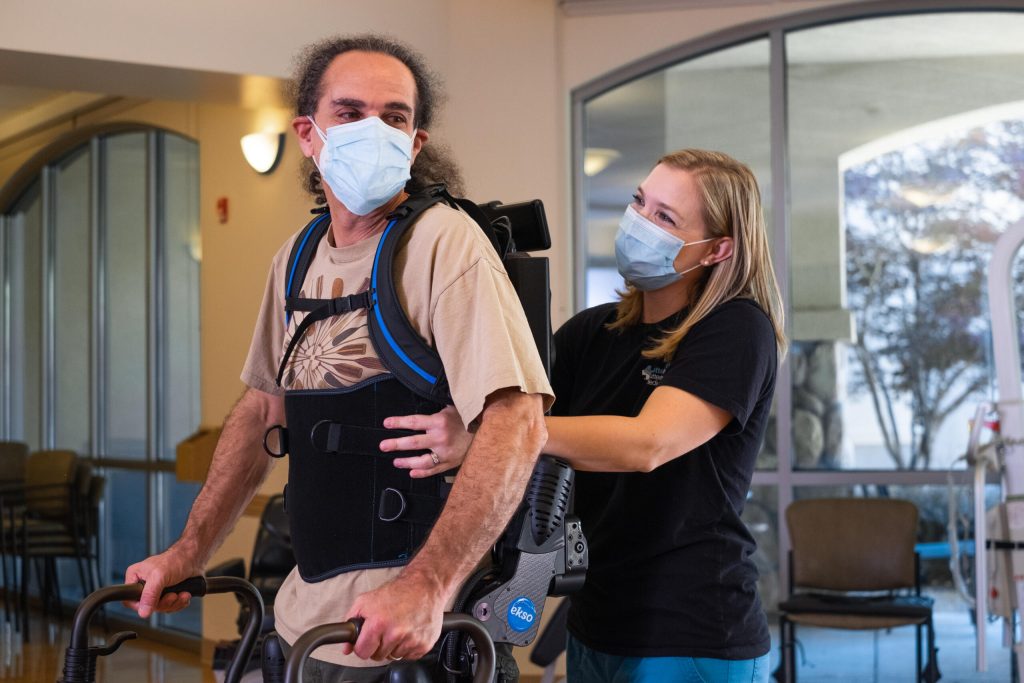
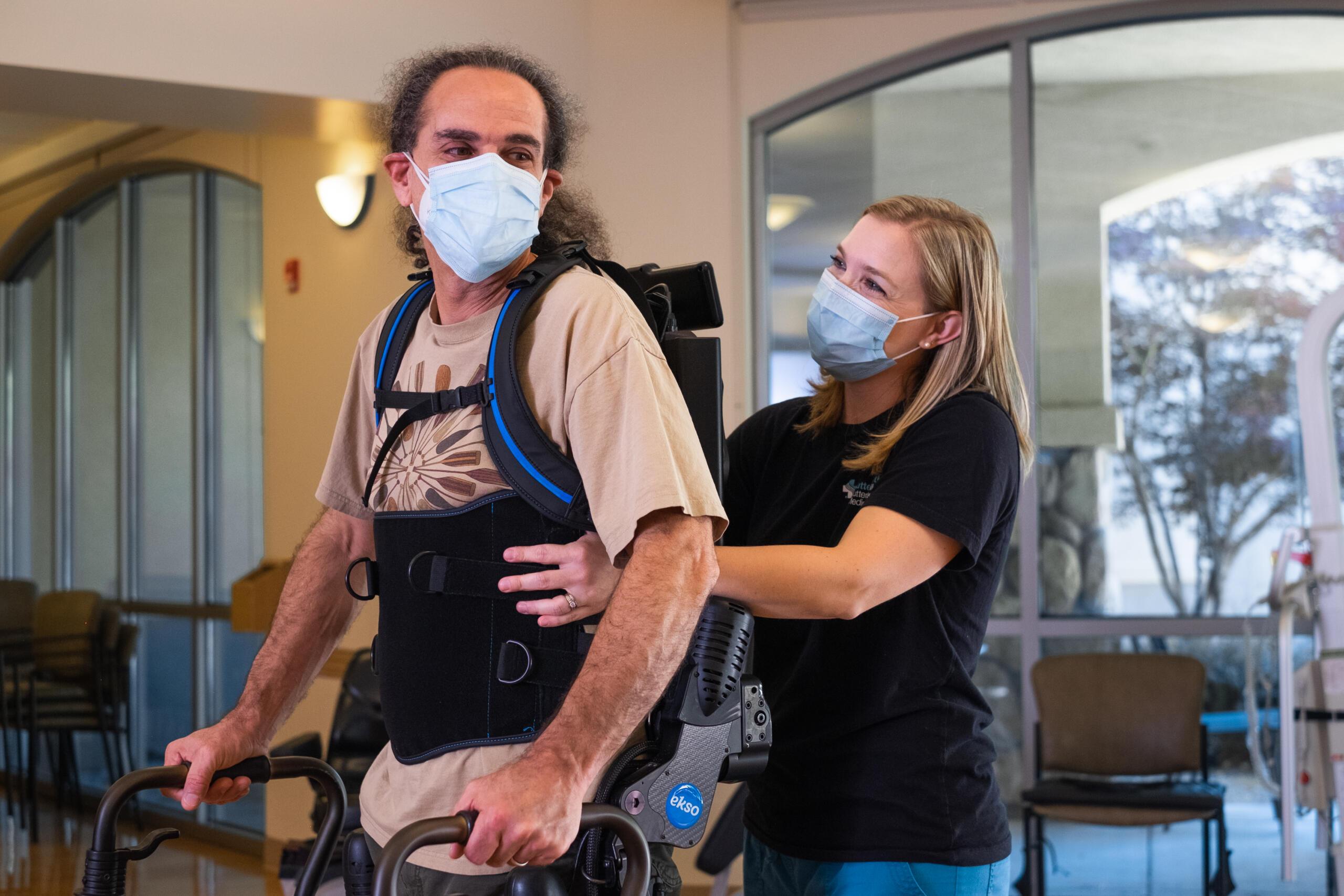
Patients with spinal cord injury exhibit a wide range of potential symptoms including: extreme pain in the neck, back, or head, urinary or bowel urgency, retention, or incontinence, abnormal band-like sensations in the thorax, impaired breathing, weakness or paralysis in upper and/or lower extremities. The use of a robotic exoskeleton can help to significantly alleviate these symptoms or, in some cases, eliminate them. The patient wears a backpack-like support which connects to robotic leg-support structures and attaches comfortably to the waist, hips, legs, and feet. This helps to support the body and protect joints during preGait and gait training.
Those who suffer from loss of mobility after a stroke or ABI can wear a robotic exoskeleton, which provides therapists the opportunity to retrain their muscles and brains to regain lost mobility. This has proven to be successful in helping thousands of patients leave their wheelchairs or walkers behind. The 2022 clinical trial (WISE), performed by The International Spinal Cord Society, focused on a 12-week exoskeleton-based robotic gait training regimen to track clinically meaningful improvement in independent gait speed among participants with chronic incomplete spinal cord injury (iSCI). The results showed that the proportion of change in the clinical ambulation category was highest among participants in the group using exoskeletons developed by Ekso Bionics. 5 of 9 participants in the “Ekso group” exhibited the greatest change in ambulation status. In comparison, only 3 of 10 within the Active Control group showed improvement in the ambulation category, and 0 of 6 in the Passive Control group displayed any meaningful change (between group difference in proportions p < 0.05, Table 5).
For the prevention of injury rather than recovery from it, those working in industrial settings such as construction and manufacturing benefit significantly from exoskeleton technology. For industrial application, exoskeletons are designed to increase productivity and reduce fatigue, with the goal of eliminating work-related injuries to the neck, shoulder, and back.
Types of Mobility Exoskeletons Target
Exoskeletons can target mobility nearly anywhere on your body—your ankles, knees, shoulders, and so on. They are generally divided into two segments: lower body and upper body.
Lower body exoskeletons are engineered for patients suffering from lower extremity paralysis or weakness and offer postural trunk support as well as support at the knee, hip, and ankle. In doing so, they may help the wearer regain their natural walking ability.
Upper body exoskeletons are designed to assist a patient’s affected shoulder or arm and have been a revolution in upper limb rehabilitation. Engineered for patients suffering from upper extremity paralysis or weakness, upper exoskeletons help patients recover strength, endurance, and range of motion.
7 Ways Exoskeletons Help Regain Mobility
Posture support
Posture has a significant impact on movement patterns and is directly correlated with a person’s ability to walk. A rigid component on the back of an exoskeleton offers support for patients with decreased trunk control. This helps them bear their own weight with proper postural alignment for maximized treatment time. Your posture is a central part of your body’s functionality, affecting the way both your upper body and lower body move, so this level of support is non-negotiable when it comes to regaining mobility.
Adaptive Gait Training
Sensors and software components of the exoskeleton continuously monitor and regulate leg movement. If a patient is leaning, the exoskeleton will automatically detect it and provide feedback that their physical therapist can use to help improve their balance and gait. The device and therapist work in conjunction to keep patients from compensating to avoid discomfort and achieve faster results.
Pre-ambulatory tools
It’s commonly known that balance plays a big role in maintaining successful mobility. If you’re struggling to keep your weight centered, walking is going to be a challenge to say the least. The pre-ambulatory tools are a suite of programs dedicated to helping patients balance, weight shift, squat, and step in place before walking. The squat function can also be used as an advanced feature to challenge patients in strengthening lower extremities.
Feedback
Resuming natural step length and swing symmetry is one of the most common goals in rehabilitation. Without proper symmetry, walking is possible. However, loss of symmetry would make walking difficult, could delay progress, and require an uncomfortable amount of effort to achieve movement. Real-time feedback helps patients regain proper step length and swing symmetry in hopes of restoring their ability to walk naturally and with ease.
Data
Regaining mobility shouldn’t be a guessing game. In order to make the necessary improvements for resuming natural mobility, a patient needs to be able to build on successes and correct any irregularities. Data tracking allows for this by showing session-specific walking time, distance, and speed in addition to symmetry, securely saved to a cloud-based dashboard for easier analytics. With smart data capture and clinician controls, medical professionals can evaluate patients and their training sessions in real-time to best help each individual on their road to recovery.
Assisted Motion
By providing the proper support, exoskeletons can boost the range of motion being used to regain mobility. For example, the Ekso Bionics upper-extremity exoskeleton offers assistance to the shoulder and arm on all planes. As a result, the patient can exercise 180 degrees of motion where they otherwise may not be able. It also allows for a more natural movement pattern by supporting the limbs with minimal interference.
Robotic Powered Movement
With powered exoskeletons, the robotic power itself can drive significant results in the process of regaining mobility. The bionic components can provide total support and trajectory assistance for patients with complete paralysis. Patient-initiated movements can be used to encourage muscle activity for those with remaining strength and the sensors will register that initiation and assist the patient in carrying out the movement – only as much as the patient requires.
Alternative Methods of Treatment Alongside Exoskeletons
Depending on the diagnosis that led to a loss of mobility, there are a number of different kinds of treatment approaches that your physical therapist may use in conjunction with the use of exoskeleton technology to aid in the rehabilitation process.
Individuals with loss in mobility due to disease or an injury sustained by the nervous system may need a physical therapist who specializes in neurology to evaluate and contribute to a full recovery.
Elderly patients, whose mobility is declining due to age, may benefit from geriatrics in addition to their exoskeleton treatment. Likewise, adolescents with inherited illnesses or injuries should supplement their exoskeleton treatment with physical therapists who specialize in pediatrics. There are also specialized therapists for sports-related injuries and women’s health.
Why Choose Ekso Bionics Exoskeletons?
Since 2005, Ekso Bionics has used exoskeleton technology to enhance natural abilities and improve quality of life. We are the leading exoskeleton company to offer technologies that help those with paralysis stand up and walk, enhance worker capabilities globally, and provide research for the advancement of R&D projects intended to benefit U.S. defense capabilities.
As the first exoskeleton FDA-cleared for acquired brain injury, stroke, and spinal cord injury, EksoNR offers the industry’s most natural gait, re-teaching the brain and muscles how to properly walk again.
Conclusion
If you or a loved one is suffering from imparied mobility after a stroke, brain injury, or spinal cord injury do not hesitate to get the best possible care. Consider the pros and cons of using human robotic exoskeletons in the rehabilitation process and do your research to find out if they are right for you.
As one of the top trends in the health and tech industries today, human robotic exoskeletons are reshaping our approach to both medical treatment and industrial labor. On one hand, robotic exoskeletons are bringing hope to people across the world who are dealing with the loss of mobility and independence or suffering from paralysis after a stroke, brain injury, or spinal cord injury. On the other hand, they are enhancing worker capabilities beyond what was previously thought possible. Considering the nature of their advantages, it shouldn’t come as a surprise that they are also being used in military research and development.
What are Human Robotic Exoskeletons?
Human robotic exoskeletons are mechanically made, taking a user’s anatomy into consideration, to improve mobility and endurance. They involve the application of robotics and bio-mechatronics — a study of science that merges biology with “mechatronics”, a discipline at the crossroads of electronics, mechanics, and computing. The focus of this groundbreaking technology is to increase bodily independence and effectiveness. It is designed to assist humans by enhancing, reinforcing, or restoring, depending on the circumstances, an individual’s physical performance. Human robotic exoskeletons can also work to reduce the energy it takes to move joints, making repetitive tasks easier, and also work to improve human movement in cases of mobility loss.
The earliest work related to human robotic exoskeletons was much earlier than you might think. A Russian inventor named Nicholas Yagn had the first approved patent for a powered exoskeleton in 1890. It was a spring-operated device designed for the military with the intention of enhancing a user’s ability to run and jump, but it never made it past the drawing board.
Finally, around the year 2000 came BLEEX (Berkeley Lower Extremity Exoskeleton), a pair of robotic legs designed by engineers at UC Berkeley and funded by DARPA (Defense Advanced Research Project Agency) aimed at lessening the effort it takes to carry heavy loads over long stretches.
Today, robotic exoskeletons have become more prevalent and complex, with an array of functions and uses. Companies like Ekso Bionics have designed exoskeletons for the purpose of military research, assisting industrial labor, and aiding neurorehabilitation.
Components of Human Robotic Exoskeletons
Robotic exoskeletons made for humans may look different depending on the functions they serve. Exoskeletons can be made from materials such as carbon fiber, metal, and elastic. Their coverage also varies from the entire body, to lower or upper extremities, or to a specific body part like the shoulder, hip, or ankle. Some exoskeletons have adjustable hardware so they can be tailored to the individual that is using them. Overall, the technology behind the exoskeleton depends largely on its type and function.
There are two types of exoskeletons: powered and passive.
Powered exoskeletons are equipped with electronics that register how much force is being applied to any given action, allowing the exoskeleton to share some of that burden with the user. In order for the exoskeleton to work properly, there must be technologies to support the three modules: sense, decision, and execution. These technologies include sensors, actuators, mechanical structures, algorithms, and control strategies that gather necessary information for carrying out each action. It may sound complicated, but it’s actually fairly straightforward. There are three basic steps that accompany the three modules.
The sense module is where the information gathering takes place. The exoskeleton records data from the user via the device sensors.
Next, the decision module interprets that data and sorts it into the intended activities.
Finally, the execution module provides the mechanical power to complete the task.
This feature allows the user to view session-specific walking time, distance, and speed. It also securely saves this information into a cloud-based dashboard for easier analytics.
Clinician control:
This feature allows the clinician to set certain parameters they can use to help better assist their patient, ushc as training targets and step parameters.
Smartassist software:
This feature allows the clinician to customize motor support independently on each leg for various impairment levels, from full assistance to patient-initiated movement, in both swing and stance phases of walking.
Adaptive gait training:
This feature consists of sensors and software continuously monitoring and regulating leg movement to minimize compensatory gait patterns.
Pre-ambulatory tools:
The feature possesses a program suite called preGait that consists of programs that help patients balance, weight shift, squat, and step in place before walking.
The exoskeleton vest was built with a patented stacked-link structure that seamlessly follows the user’s arm and elbow through the full range of motion while providing proper joint alignment through repetitive movement.
Extreme logistics positions
These positions include reaching directly overhead, across the body, or even into a back pocket for a phone — are unrestricted with this wearable exoskeleton.
Adjustable, high-force actuators
These actuators are proven to be extremely durable with over a million cycles before requiring replacement.
Customized Assistance Levels
The level of each device can be adjusted for the user and task by easily swapping out the set of compact gas springs. Different levels can even be selected for each arm independently depending on the task.
Passive exoskeletons are purely mechanical, providing support using pulleys, a spring balancer, and weights to counterbalance the workload. Passive systems generally take the weight off the user’s shoulders and arms and transfer it to their center of gravity so that the user obtains increased endurance during overhead tasks and other demanding work.
Exoskeleton technology not only helps the individual perform tasks that directly aid in increasing mobility, but also provides medical professionals with the information needed to offer treatment with a higher chance of success. For patients with a low likelihood of regaining their mobility, these machines can be a saving grace, in many cases enabling full rehabilitation.
Exoskeletons for Rehabilitation
Diseases or injuries that can be treated with physical therapy and a wearable exoskeleton include but are not limited to: stroke, spinal cord injury, traumatic brain injury, aneurysm, hypoxia/anoxia, ischemia, brain tumor, or any other acquired brain injury. For individuals recovering from these injuries, exoskeletons are great for rehabilitation and mobility restoration. Exoskeletons have the potential to bring these patients from lower limb disability and complete loss of movement all the way to the point of getting out of their wheelchairs, and learning to walk again. One study from 2015 found that, “The ability to restore gait for individuals with paraplegia has improved with progress in various powered exoskeletons and neuromuscular stimulation technologies. The powered exoskeletons are able to restore the stand up, sit down, and walking motions.” These human-augmenting devices are truly a rehab tool for physical therapists to challenge their patients, requiring active participation known to drive brain plasticity.
Exoskeletons for Upper Extremity Therapy
Upper-extremity rehabilitation exoskeletons assist physical therapists, occupational therapists, physiatrists, and doctors in clinically rehabilitating patients with upper-body weakness or paralysis. This new technology also greatly benefits industrial applications and other workplace settings or job sites. Wearable exoskeletons help workers complete tasks with full range of motion rather than giving in to fatigue, overuse, or repetitive movements.
An injury resulting in decrease of upper-body strength can come from any number of areas whether that be occupation risks, sport injury, or illness. An upper-body exoskeleton is a wearable vest that helps you perform everyday tasks and use your arms and shoulders without limitations. There are a few different reasons why someone may benefit from upper-extremity therapy and bionics. Some conditions EksoUE is beneficial for include: stroke, spinal cord injury, traumatic brain injury, muscular dystrophy, ataxia, orthopedic injury, Guillain barre, brain tumor, brachial plexus injuries, and other upper-extremity weakness or paralysis. Rehabilitative treatments may begin immediately post-injury or after any chance of reversing the damage through medical means has passed. These treatments are designed to strengthen weakened muscles, reteach parts of the brain to take over for the damaged areas, and help the patient adapt to a new way of doing things.
Exoskeletons for Lower Extremity Therapy
Exoskeletons for lower extremity therapy are appropriate for many people recovering from spinal cord injury, stroke, and brain injury at any stage of in-patient or outpatient rehabilitation, preferably as soon as possible after diagnosis. It can be helpful for patients to stand and take their first steps post-injury and retrain brain and muscle function as they learn to walk again. It can also help fine-tune walking skills and help improve patients’ gait as they learn to regulate their movements.
With this tool, patients have the opportunity to gain as many lost abilities as possible. The exoskeleton provides progressive levels of support so the clinician can reduce the assistance the system offers patients as they improve, and can even add resistance to one or both legs. Patients who use a wheelchair can use the exoskeleton to regain the ability to stand, retraining muscles to support body weight without strain. Therapists toggle between patient-initiated and therapist-initiated movement, tailoring rehabilitation to the patient.
Human Robotics for Industrial Labor
Industrial workers in construction or manufacturing benefit from a significantly lower likelihood of injury and increased quality of work by using exoskeletons to enhance their physical capabilities. Mechanical arms and vests help them lift heavy loads and perform repetitive tasks through an active range of motion so they can avoid giving in to fatigue and/or injury.
Why Choose Ekso Bionics for Human Robotic Exoskeletons?
Ekso Bionics is the leader in exoskeleton technology with the first FDA-cleared exoskeleton for both stroke and SCI in addition to acquired brain injury. With more than 175 conference presentations, chapters, and published articles, Ekso is the most widely-studied exoskeleton for rehabilitation, progressing patients far beyond what they would otherwise be able to accomplish. Our exoskeletons are backed by data from over 40 industry-leading research partners and help those with paralysis to stand up and walk, enhance worker capabilities globally, and provide research for the advancement of R&D projects intended to benefit U.S. defense capabilities.
Industries Ekso Bionics Specializes In
EksoHealth is the arm of Ekso Bionics that specializes in neurorehabilitation. We have helped thousands of patients with lower extremity disabilities take over 180 million Ekso-aided steps and have inspired an entirely new medical device industry. Similarly, we have helped many patients with upper extremity disabilities, allowing them to achieve rehab sessions with a higher dosage, more intense therapy, and a wider active range of motion.
EksoWorks is the arm of Ekso Bionics that specializes in our exoskeleton technology for industrial applications. Our EksoWorks upper-body lifting exoskeletons were designed to increase productivity and reduce fatigue, with the goal of eliminating work-related injuries to the neck, shoulder, and back.
Conclusion
Whether you’re looking to regain mobility, increase your capabilities on the job, or prevent injuries, human robotic exoskeletons are a reliable and technologically safe choice. We hope our exoskeletons provide you support and progress in rehabilitation and lower the number of worker-related injuries for years to come.
Strokes are the fifth leading cause of death in the United States and a major cause of long-term disability. Thankfully, great strides have been made in treating patients who have had strokes and been left with a disability. Ekso Bionics is leading the way with robotic exoskeletons to help those who have lost mobility due to stroke, spinal cord injury, or brain injury regain what they have lost.
What Is a Stroke?
A stroke occurs when part of the brain is deprived of oxygen. This can be caused by a blood clot blocking blood flow or by a rupture in the artery feeding blood to that part of the brain. Either way, if blood flow is not returned to the affected part of the brain quickly, the damage to the brain can become permanent. This can result in varying degrees of disability or death.
There is also a type of stroke that is temporary. Known as a transient ischemic attack (TIA), these happen when the blood supply to the brain is cut off for only a short time. After experiencing a TIA, a patient may become clumsy or confused, but the effects are only temporary. Once blood flow returns to the brain, the effects of the TIA dissipate. It is still vital to see a doctor after having a TIA. People who frequently have these attacks may have a full-blown stroke later on.
Immediate treatment can sometimes reverse the effects of a stroke. In the case of permanent stroke damage, rehabilitation with EksoNR exoskeleton can successfully return patients to a lifestyle similar to the one they enjoyed previously. You can read more about the research on EksoNR and stroke in our Clinical Summary. This transformative device has been helping adults of all ages regain their mobility and their quality of life.
Health Effects of a Stroke
Because the brain controls almost all of our bodily functions, the range of effects from a stroke is very broad. Frequently, patients who have had a stroke have complete or partial paralysis to one side of their body, including the facial muscles. This can manifest as drooping eyelids, an inability to speak or chew food properly, and reduced mobility.
Sometimes strokes do not affect a person’s limbs and muscles but rather the parts of the brain that control thinking, speech, hearing, or eyesight. In these cases, a patient may have a diminished ability to think clearly or logically. They may show personality changes or lose their memory. If the areas of the brain that control the senses are damaged, the result may be loss of taste, smell, hearing, or sight.
Even with advances in understanding strokes, it is still somewhat unpredictable how a stroke will affect someone. If the patient’s symptoms include decreased mobility, even if it is severe, EksoNR robotic exoskeleton can be a powerful tool for reversing this potentially life altering side effect.
Stroke Treatments
Stroke treatments fit into two categories: preventative treatments and rehabilitative treatments to regain what was lost.
Preventative Stroke Treatments
Immediate stroke treatments vary depending on how the stroke occurred. If a blood clot caused the stroke, then medications will be given to thin the blood and reduce the size of the clot. If a rupture or other brain bleed caused the stroke, steps would be taken to stop the bleeding and return blood flow to that part of the brain.
In both instances, medication is often given to reduce the patient’s blood pressure. High blood pressure can be both a cause and a result of a stroke.
Rehabilitative Stroke Treatments
Rehabilitative stroke treatments begin after any chance of reversing the damage through medical means has passed. These treatments are designed to strengthen weakened muscles, reteach parts of the brain to take over for the damaged areas, and help the patient adapt to a new way of doing things. While physical, speech, and occupational therapy is a part of these treatments, new technology, like EksoNR, gives patients who have had a stroke that resulted in paralysis or loss of mobility more options, and hope.
EksoNR is a robotic exoskeleton that the Food and Drug Administration has cleared for rehabilitation after stroke. It provides therapists the opportunity to work with patients’ brain plasticity and retrain their muscles and brains to regain lost mobility. It has shown great success at helping thousands of patients leave their wheelchairs or walkers behind.
EksoNR can be utilized both in walking and preGait modes. Pre-gait activities include those that work on balance, midline orientation, and prepare a patient for walking.
The various gait-training modes offer support to the torso, hips, knees, and ankles while keeping the patient in a fully upright posture and providing varying amounts of power to one or both legs. EksoNR uses a gyroscope, sensors, and software that monitors the position of the EksoNR to ensure that training is done effectively and safely. As a patient progresses and regains midline orientation, coordination, and strength, EksoNR will reduce the output of power allowing the patient to progress so they can walk out of the device.
The patients who use EksoNR exoskeletons post-stroke are kept apprised of their progress and must actively participate in the process to succeed. This might look like assisting with weight shifts, and may progress to the patient controlling all aspects of the steps they are taking. This involvement and positive progress reports can have a profound psychological effect on the patients, increasing their odds of improving outcomes.
A stroke is a medical emergency, capable of damaging the brain through interruption of its blood supply. There are many symptoms of stroke including difficulties walking, speaking, and understanding, as well as numbness of the face, arm, or leg. When it comes to treating subacute stroke in an inpatient rehabilitation setting, Dr. Crissy Voigtmann (Doctor of Physical Therapy and board-certified Neurological Clinical Specialist), Dr. CJ Curran (Doctor of Physical Therapy, certified brain injury specialist and board-certified Neurological Clinical Specialist), and Jose Dominguez (Director of Rehabilitation, Orlando Health) give professional insight on EksoNR, the first FDA-cleared exoskeleton for stroke and spinal cord injury, and the only FDA-cleared exoskeleton for acquired brain injury.
Orlando Health ORMC Institute for Advanced Rehabilitation (IAR) is a CARF accredited inpatient and outpatient rehab unit partnered with Ekso Bionics since 2019. Currently, they have four Level-Two trained therapists at the inpatient rehabilitation, and two Level-Two trained therapists at their outpatient rehabilitation.
What is EksoNR?
Currently, EksoNR is the only exoskeleton that is FDA-cleared for acquired brain injury. It is the first FDA-cleared exoskeleton and extremely adaptive with short-term implications as well as long-term ones. The device is capable of progressing through programming as a stroke patient progresses in recovery. This gives the long-term capability to adapt from session to session, not only for patients with strokes but spinal cord injuries or TBI.
Who can benefit from EksoNR?
In 2020, IFR had 310 stroke patients arrive at the unit. On average, they had a 1.58 acuity level, based on a case-mix index equation that determines the acuity level for inpatient rehab. Typically a stroke patient stayed at the unit for 15.7 days. In order to determine mobility scores upon admission, Crissy and CJ used Care (formerly known as FIM), which is a standardized test that all inpatient rehabilitation facilities have to use for all diagnoses.
Additional Care scores from the facility include:
Average Care Score: 2.9 (Max Assist)
Average Walking Score (per 50ft): 2.2 (Max Assist)
Average Walking Score (per 150ft): 1.7 (Total Assist)
Average Stair Score: 1.2 (Total Assist)
At IAR, these scores were what the average numbers looked like for all stroke patients and are important to know to where those who used Ekso started from at baseline.
[The following is condensed from the full webinar of Dr. Crissy Voigtmann and Dr. CJ Curran.]
What were the deciding factors in having Ekso a part of the program at Orlando Health?
As Dr. Crissy Voigtmann and Dr. CJ Curran were in the decision-making process of having Ekso become a part of their program, they were asking themselves: “Are we doing enough? Are we providing these patients with enough repetitions at a high enough intensity level to elicit the neural change that needs to happen during this short length of stay that we have?”
In general, the answer to the questions they asked was no. They ultimately decided there was not an exact dosage that has been established for intensity or for repetition, but there was a growing body of evidence that demonstrates for gait in particular; that stepping practice needs to be in the thousands a day for optimal improvement.
Observational studies have shown that in inpatient rehab facilities (places that have stroke programs), stroke patients are taking an average of 250 steps a day. To further reinforce that point, these same studies have shown that stroke patients on average spend greater than 50% of the day in bed and greater than 60% of their time alone.
Not only were they not utilizing the active time with these folks to provide high-intensity therapy that is necessary for neural training, but even during the passive time, they realized they were not providing the necessary environment, whether it be with engagement or stimulation that is necessary for improvement as well.
They determined the best solution was integrating Ekso into their program. This was the bridge. This bridged the gap between that dilemma and that solution. For them, Ekso allowed them to accomplish those goals on day one and early, especially for their folks who are significantly impaired, the ones with a lot of deficits. These were folks, in their experience, that are really difficult to gait train. These are the people that unfortunately tend to fall through the cracks and would get low level therapy or low intensity therapy otherwise.
How has Ekso changed training for the patients?
Because of Ekso, they were able to get individuals up early and on their feet for extended periods of time, participating in high-intensity therapy from the very beginning. There are certain positions that would take two or three therapists, or three pairs of hands, to get a patient to accomplish. But one therapist is able to do it whilst focusing on other deficits as well, thanks to Ekso.
Who are the candidates for Ekso?
The stroke patients primarily receiving early Ekso intervention:
Dense Hemiparesis: 0-⅖ MMT throughout affected lower extremity
Pusher Syndrome
Significant Postural Control and Awareness deficits
Motor planning and Sequencing deficits
Other patient specific factors leading to early Ekso utilization:
Obesity/Height (under 220lbs, under 6’5” approximately)
Impulsivity
Cognitive deficits
The overall message is these patients are individuals who are very difficult to manually facilitate. They are very difficult to provide the manual techniques that are necessary to hit high repetitions or to hit high intensity levels. As a result, they are going into the exoskeleton.
[The following is condensed from the full webinar of Dr. Crissy Voigtmann and Dr. CJ Curran.]
The Institute For Advanced Rehabilitation (IFR, Orlando Health) is a CARF accredited inpatient and outpatient rehab unit partnered with Ekso Bionics in 2019. With the utilization of EksoNR (the first FDA cleared exoskeleton) in the rehabilitation of patients, they were able to narrow down the typical patient profile and measure their progression via outcomes from using EksoNR.
Average Stroke Patient Statistics
The following data represents the “average” scoring of all of their 310 stroke patients. It is provided so that anyone may look over and compare this data with those they tended to put into the exoskeleton. When patients are referred to as going into the exoskeleton, please note that it means at the exoskeleton’s maximum assistance level.
Now, their outcome measures. The postural assessment scale for stroke (PASS) is a stroke specific outcome measure that is determined by movement of the patient: they’re sitting, they’re rolling in bed, they’re standing, and then picking up something off the floor, as well as single limb stance. Typically that score is out of 36. Their average PASS score on admission for all patients with stroke was a 20.7, which indicates significant deficit. 12.4 is the average PASS score for their stroke patients going into Ekso, so they are even more impaired than the average patient they saw on the floor.
The Berg is out of 56 with the benchmark being 45; you can see the patients come in a lot lower level than that at 16.6. The Berg for the exoskeleton candidates is 4.9, meaning they can sit and maybe be transferred by one person – that’s generally a five out of 56 on the Berg. Some patients who get into the exoskeleton can sit independently and some cannot; again, as you can see reflected in the data, their gait is almost not a gait. It is very, very slow, 0.04 meters per second, if they are even ambulatory.
Average Care Score for Mobility on Admission for all CVA:
Transfers: 2.9
Gait: 2.2 for 50 feet and 1.7 for 150 feet
Stairs: 1.2
Average Outcome Measure Performance on day of evaluation for all CVA
PASS: 20.7
BBS: 16.6
10 MWT: 0.24 m/s Self Selected Speed and .33 m/s Fast Speed
Average Care Score for mobility on admission for patients using ekso:
Transfers: Total (1)
Gait: Total (1) for all ambulation
Stairs: Total (1)
Average Outcome Measure Performance on day of evaluation for patients using Ekso
PASS: 12.4
BBS: 4.9
10 MWT: 0.04 m/s Self Selected Speed and 0.04 m/s Fast Speed
How often is the exoskeleton used on the floor?
Generally, given that their length of stay is about 15 days, they were (on average) getting people into the exoskeleton four times during their stay. However, that really depends on the type of patient and their situation. They have had people in as many as 12 times during their stay.
The average number of total steps taken per patient during their stay is 1,354 with an up and walking total of at least 11 minutes per session, but the average uptime is more than half the session. That means more than half of the session is where the patient is actually standing and in a weight bearing position. They may be working on pre-gait activities. They may be working on just standing tolerance and co-treating with OT or speech. So they do utilize it longer than that 11 minutes, but that’s active walking time.
What were the deciding factors in having Ekso a part of the program at Orlando Health?
As Dr. Crissy Voigtmann and Dr. CJ Curran were in the decision-making process of having Ekso become a part of their program, they were asking themselves: “Are we doing enough? Are we providing these patients with enough repetitions at a high enough intensity level to elicit the neural change that needs to happen during this short length of stay that we have?”
In general, the answer to the questions they asked was no. They ultimately decided there was not an exact dosage that has been established for intensity or for repetition, but there was a growing body of evidence that demonstrates for gait in particular; that stepping practice needs to be in the thousands a day for optimal improvement.
Observational studies have shown that in inpatient rehab facilities (places that have stroke programs), stroke patients are taking an average of 250 steps a day. To further reinforce that point, these same studies have shown that stroke patients on average spend greater than 50% of the day in bed and greater than 60% of their time alone.
Not only were they not utilizing the active time with these folks to provide high-intensity therapy that is necessary for neural training, but even during the passive time, they realized they were not providing the necessary environment, whether it be with engagement or stimulation that is necessary for improvement as well.
They determined the best solution was integrating Ekso into their program. This was the bridge. This bridged the gap between that dilemma and that solution. For them, Ekso allowed them to accomplish those goals on day one and early, especially for their folks who are significantly impaired, the ones with a lot of deficits. These were folks, in their experience, that are really difficult to gait train. These are the people that unfortunately tend to fall through the cracks and would get low level therapy or low intensity therapy otherwise.
A Case Study with EksoNR
Almost 60% of the patients are stroke patients. They found that the EksoNR does such a good job, that typically they’re ambulatory at the end of their rehabilitation, and they move on to their outpatient clinic. An incomplete spinal cord would be their second highest diagnosis in terms of volume.
Take into consideration the progress of one of their patients, Sarah. She is a 62 year old female. She had multiple ischemic strokes in her right hemisphere. She also presented with pusher syndrome. With pusher syndrome, the difficulties that arise in therapy are because of misunderstanding of midline orientation: they are persistently laterally leaning, and/or they’re pushing themselves over onto their weak side. This is very challenging to treat because they are going towards a limb that is hemiperetic and does not support their body. Just getting that patient to take a step is difficult because their weight shifting is so impaired.
Sarah is also a tall and large woman, which makes it even harder for a therapist to facilitate gait. She had left neglect. Her admission was very early after her stroke, just five days post-stroke, so all of the therapy was new for her. In addition to her challenges, she was also a braille user.
Her admitting outcome measure scores PASSwas a 12 out of 36, and she was non-ambulatory, requiring maximal assistance for her bed mobility and her transfers, while being dependent for gait. They were able to get her in the Ekso three times. She didn’t take a ton of steps. They were a little bit limited in her length of stay and her time, but these steps were very effective and these sessions were very effective. They allowed the exoskeleton to facilitate those steps. When they put on the Ekso, it was just one therapist and the tech or an aide. They were able to spend more time standing doing pre-gait. The clinicians were treating that pusher syndrome by having her shift her weight onto her limb more. They recall that was a significant moment for this patient.
The data for her outcome scores are below so that you can compare her admission to her discharge:
Admission:
BBS: 5/56
PASS: 12/36
10 MTW: 0m/s
Max A bed mobility and transfers; dependent for gait
Discharge:
BBS: 17/56
PASS: 29/36
10 MTW: SS 0.15m/s; FP 0.15m/s
SBA Bed Mobility, SBA for 10 feet of gait and transfers, Min A gait >150 feet and 4 stairs
Crissy Voigtmann received her Doctor of Physical Therapy from the University of St. Augustine in 2014. She’s a board certified neurologic clinical specialist. She works as a full-time clinician serving patients with brain injury, stroke, neuro oncology, and incomplete spinal cord injury, and spearheads program development for locomotor training for all neurologic patients in the inpatient rehab setting at Orlando Health’s Institute for Advanced Rehabilitation.
What were the first steps toward introducing EksoNR in a rehab program?
When the doctors at Orlando Health first got the exoskeleton, they were collaborating and came up with this idea of having a lead locomotor person. Dr. Voigtmann became the lead person just to help bridge the gap between their non-Ekso therapists on the floor, with either pairing them with an Ekso therapist or with Dr. Voigtmann herself. They were afforded that ability just by creating the role of lead locomotor therapist at the clinic.
The other first step was a designated area off to the side of the gym, so that the exoskeleton has everything there that it needs. There you will find all evaluation forms and data collection sheets and the measuring tools. Everything is in one spot, so that if someone thinks, “This is a great patient for Ekso. I want to do quick measurements,” the opportunity is available to them. They get that patient on the mat, take the measurements, and that allows them the opportunity to get the patient into the Ekso the next session if the current session is unavailable. They have found that it is a nice way to keep everything in one place.
How do you refer patients to EksoNR?
They tried to come up with a referral system. For example, their unit has nine teams, so nine teams of PT/OT and they only have four Ekso-trained therapists. What do they do with the other teams? They paired up with an Ekso clinician in order to have the opportunity to propose, “Can we switch this patient off? You see one of mine and I’ll see one of yours.” With this method, they could optimize the number of patients getting into the exoskeleton and get the benefits of early gait training.
What else has helped EksoNR be successful in inpatient rehab?
At IFR, they have been very fortunate to have really engaged rehab aides in their unit. They went through training sessions with them on how to do wrenching techniques, how to size the Ekso, how to clean it, and even sometimes how to write down some of the data on a data collection sheet for them if time is critical.
They have been essential in the setup, the breakdown, and taking all of the information. They’re also really skilled at using the Ekso controller so that they don’t have to pull in too many more people. Essentially, there would be a physical therapist who is Ekso-certified and then a tech for each session. That really helps to make it effective; cost efficient for the company, and also time efficient.
The stroke patients primarily receiving early Ekso intervention:
Dense Hemiparesis: 0-⅖ MMT throughout affected lower extremity
Pusher Syndrome
Significant Postural Control and Awareness deficits
Motor planning and Sequencing deficits
Other patient specific factors leading to early Ekso utilization:
Obesity/Height (under 220lbs, under 6’5” approximately)
Impulsivity
Cognitive deficits
The overall message is these patients are individuals who are very difficult to manually facilitate. They are very difficult to provide the manual techniques that are necessary to hit high repetitions or to hit high intensity levels. As a result, they are going into the exoskeleton.
[The following is condensed from the full webinar of Dr. Crissy Voigtmann and Dr. CJ Curran.]
While EksoNR (the first FDA-cleared exoskeleton for ABI, stroke and spinal cord injury) is a technological advancement that has changed the way patients with stroke experience rehabilitation, it is not without its own difficulties. The Institute For Advanced Rehabilitation (IFR, Orlando Health), has been partnered with Ekso Bionics since 2019. Dr. Crissy Voigtmann and Dr. CJ Curran utilized EksoNR with certain patients and found some difficulties that they were not at first prepared for.
The Generation Gap
With stroke comes increased age. Typically speaking, some of the older individuals are not as comfortable with technology. It becomes very apparent once they get into EksoNR and they’re fearful. Their anxiety can become a pretty significant barrier to try to get them acclimated to this level of technology. Not only that, but also from a deficit standpoint, individuals that have attention deficits or engagement deficits just want to go along for the ride once they are in the suit, and it can be really tough to get them to actively engage in the process of their rehabilitation.
The patients are motivated, they want to do it, but as they tried to convey what the suit is capable of or what the progression looks like, some of the patients really struggle to grasp what that next step is or what that progression will be.
Another element that caught them off guard initially was incontinence. A lot of patients have not been up against gravity for an extended period of time in a while. That has been something that they have prepared for now, and especially in advance, before they even start the session(s).
How do you fix the challenges that patients face with EksoNR?
Luckily most of the issues faced are solved through individualized education, demonstration of the device, or even allowing the patients to observe other stroke patients get into the device and complete a gait training session.
They have also implemented slow gradual exposure. Sometimes that looks like doing the evaluation, they get them up, and all they do for that session is weight shifting. It might not have been what the clinicians had planned that day, but it got then the buy-in they needed so that they could do a full gait training session the next day.
As an inpatient rehab unit, they are very fortunate to work as an interdisciplinary team. Sometimes the solution has been doing co-treats with occupational therapy or with speech therapy, or even neuro-psychology depending on what the root causes for the difficulty of the patient to engage with the device and complete the session that they needed them to.
What are the most difficult barriers to overcome?
The patient specific barriers are the most obvious, but they have found that it’s sometimes the environmental or the clinical barriers that are the most difficult to overcome. Some environmental and clinical barriers can be as concrete or as tangible as spatial limitation, but they can also be as difficult to solve for a variety of different reasons such as scheduling issues or time constraints.
EksoNR is a mechanized exoskeleton that aligns with the wearer’s anatomy to provide the support and assistance they need during rehabilitation. EksoNR is the first and only exoskeleton for ABI rehabilitation to be cleared by the FDA. It fits snugly over the patient’s legs, feet, hips, and waist to support their weight and joints.
Designed by clinicians for clinicians, EksoNR is the most widely studied rehabilitation exoskeleton available. As of July 2020, there are 74 completed clinical research studies and countless publications and white papers involving EksoNR. These studies contain the personal experiences of more than 1,800 participants around the world.
Read how EksoNR has helped one of our users regain her mobility and walk again.
Kylie’s Rehabilitation
After Kylie was injured in 2019, she went into a coma. According to Dr. Kenneth Shapiro, who specializes in Physical Medicine and Rehab, her condition was serious. She had an ABI in addition to multiple internal injuries. She recovered consciousness and soon began physical therapy. Kylie was able to regain amazing levels of self-initiated movement with the help of the EksoNR bionic exoskeleton.
Her physical therapist, Erin, related that Kylie regained much of her mobility using the EksoNR exoskeleton. “In the first session, we took maybe ten steps,” Erin shared. “And now she’s walking over 1,200 steps.” This sort of progress is spectacular in patients with ABI injuries. Considering the extent of Kylie’s injuries, this may not have been possible without EksoNR.
EksoNR has helped Kylie maintain her muscle condition and start walking again using the power of brain plasticity. With Erin’s guidance, Kylie worked on vital skills including shifting her weight, balancing, and improving her lower extremity muscle strength while wearing the device. As her gait became stronger and more confident, Kylie shifted from relying on EksoNR to using her own muscles to walk. Eventually, she only relied on EksoNR to correct any errors she madewhile walking.
How Does EksoNR Help ABI Patients Regain Their Ability to Walk?
Kylie’s story is a great illustration of how EksoNR can help people with ABI to stand and walk again.
Unlike many other exoskeletons, which provide all or nearly all of the power needed to walk, EksoNR is designed to challenge patients. With its high, stiff back and various progressive modes, EksoNR requires active participation in the rehabilitation process, so the patient can:
Learn the most efficient and highest quality gait pattern
Develop a natural gait with secure practice
Improve their functional balance
Improve gait speed
Improve walking distance
The following features also make EksoNR for ABI the ideal choice for patients to learn to walk again:
Unique design helps the patient focus on movement and balance
Data capture allows the physical therapist and patient to view session-specific speed, walking time, and distance. This information is saved securely in cloud storage for reference and analytics. It can be used by the physical therapist to provide personalized care.
Clinician control lets the physical therapist set training goals and modify EksoNR’s support and assistance levels for each leg
Adaptive gait training uses software and sensors to regulate and observe leg movement to promote gait development and strengthening
Pre-ambulatory tools such as PreGait help patients balance, squat, weightshift, and step in place before walking
SmartAssist software helps the physical therapist customize motor support depending on the patient’s impairment level.
This featured function allowed Kylie to move from full assistance to patient-initiated movement as she regained strength and coordination
Posture support allows for easier and faster recovery by helping patients get started on their gait training sooner
Physical therapists can also use EksoNR at any stage of outpatient or inpatient rehabilitation.
Edward Cruz, a physical therapist at the University of Texas Southwestern Medical Center, recounted Kylie’s case. He believes EksoNR is “a good intervention for early mobilization [that taps] into neuroplasticity expediently and more successfully,” compared to the body-weight support treadmills physical therapists often use for patients with ABI.
Learn More about EksoNR
To learn more about how EksoNR can help patients with ABI improve their gait and regain their mobility, request a demo for your practice.
EksoNR is only one of the many wearable exoskeletons that Ekso Bionics has developed for rehabilitation. Contact us today to learn more about how we can help your practice.